There are (at least) two ways in which the word “need” is used.
One is a conditional necessity to achieve some other desired goal. There are biological needs: the “rule of threes” mnemonic is that the human body can go 3 minutes without air, 3 hours without shelter (in a harsh environment), 3 days without without water and 3 weeks without food. Then there are more conditional “needs”: if one wants to be a concert pianist one needs to practice. There is no universal need to practice the piano, just a highly rare contingent one.
A second common use of the word “need” is when your Batman obsessed friend tells you that you “need” to see The Dark Knight and gives you lots of reasons why you have this “need” (Heath Ledger’s (last) performance as The Joker, yada, yada, yada). But if you haven’t already seen The Dark Knight, released in 2008, it is probably because not only do you not “need” to see it, you don’t want to. Even at money price zero, even if it happened to be on free TV just as you sat down and turned it on, you would change the channel as it isn’t worth your two hours and 32 minutes. The real “need” is not yours but your Batman-phile friend, who wants you to do something to validate them.
The widely bandied about concept and reported empirical measures of “unmet need” for contraception are the latter, while pretending to be the former.
The Demographic and Health Survey questionnaire ask women about their current fertility preferences: do they want another child now?, do they want another child, but not now? Do they never want another child? The questionnaire also asks women if they are using modern contraception. Family planning advocates then constructed a measure of “unmet need for contraception” that included every woman who met the two criteria of: (a) did not want a child now and (b) was not using modern contraception. They then publicized their calculations of “unmet need” usually with the implication that this “unmet need” is the result of a “lack of access” and use these numbers to justify “supply side” programs to meet this putative “unmet need.”
But, like the old joke about the lawyer asking one question too many (set up line: “If you didn’t see my client bite the man’s ear off, how are you so sure he did?“) the DHS asks lots of questions to women about why they are not using modern contraception. Once look at those you realize that “unmet need” as reported is really just the projection of demographer’s needs for validation of their own views.
Leigh Senderowicz and Nicole Maloney in the 2022 Population and Development Review use women’s answer’s to why they are not using modern contraception in spite of not wanting a children now to divide reasons into into “supply side” (lack of access) and “demand side” (lack of desire) answers (see the Figure from their paper).
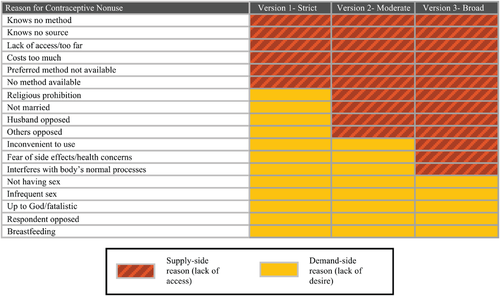
Source: Senderowicz and Maloney 2022, Figure 2.
The author’s start with the standard report of “unmet need” and then do a simple decomposition into “supply side” and “demand side” reasons across seven African countries with DHS data. They find the average of the standard reported “unmet need” is 17.7 percent. So the family planning advocates will tell you that (roughly) one in five women has an “unmet need” for contraception.
But the decomposition is: 1.4 percent is for “unknown reasons”, 15 percent is “demand side” (reasons like “not having sex”) and 1.3 percent is “supply side”. “Unmet need” due to the all six strict supply side reasons–(i) not knowing of methods, (ii) not knowing a source, (iii) lack of access/too far, (iv) costs too much, (v) preferred method not available, and (vi) no method available combined is only about one woman in 100. And this is in very poor African countries where one might think “access” is low and cost a big factor. Even in the DRC “unmet need” was 22.5 percent but only 1.9 percent of that was “supply side.”
What is striking is that the fact that “unmet need” does not reflect a woman’s reported need but rather a need imputed to women by others regardless of their explanations as to why they are not using modern contraception, is not a new finding or a “dirty little secret.” Since the data is widely available, analysts have known for a long time that very little of the high levels of officially reported (by UN agencies and others) of the reported “unmet need” is “access” related (an old (draft) paper of mine from 1996, for instance).
A recent article forthcoming in the American Economic Review by excellent economists that reports on a large RCT in Burkina Faso providing a voucher to cover 100 percent of the costs of contraception for the “treatment” group.
They frame the experiment in the context of the “delayed” fertility transition in Sub-Saharan Africa. The say that “arguably the most influential view is that limited access to affordable contraception is the key driver of high fertility in Sub-Saharan Africa.” “Under this view, there is a large “unmet need” for contraception: many pregnancies are unintended and could be prevented if women had access to reliable and diverse birth control methods.” Their footnote 1 is: “This view is supported by the fact that 20 to 40 percent of women in low income countries report not wanting to get pregnant in the near future, yet they are not using any modern contraception method–this is the definition of “unmet need.” So they take the concept of “unmet need” completely uncritically.
But this is just set up as their results destroy the plausibility of the “most influential view.” The basic result is that there was no significant effect (either statistically or practically) of women having received a voucher to cover contraception costs. The first row of the table (take directly from Table 2 in the paper) shows the result for the whole, very large, sample. Women who received the voucher that covered 100 percent of contraceptive costs were only 1.9 percent less likely to have a pregnancy over the next three years than the control group, who received a voucher covering only 10 percent of the costs. While 70.5 percent of the control group had a pregnancy over the three years the participants were tracked so did 68.6 percent of the treatment, 100 percent subsidy women. Even with the very large sample the standard error of .012 means that the hypothesis that the effect of the subsidy was zero cannot be rejected at conventional significance levels.
| Sample | Results | Had a live birth since baseline | Had a pregnancy since baseline | Used medical contraception in last three years |
| Full Sample (with controls, province fixed effects) | Estimate Std. Err. N Control mean | -.017 (.012) 12,542 .623 | -.019 (.012) 12543 .705 | .0003 (.015) 12,131 .531 |
| Had unmet need for contraception at baseline | Estimate Std. Err. N Control mean | -.011 (.015) 4649 .662 | -.015 (.014) 4649 .736 | .018 (.019) 4659 .437 |
| Wife did not want another child over the next 2 years at baseline | Estimate Std. Err. N Control mean | -.016 (.013) 7583 .611 | -.021 (.013) 7583 .703 | .009 (.017) 7583 .559 |
What is even more compelling is that the authors look at the subsets of women who, on the “unmet need” conjecture would be the most responsive to the subsidy. The second row of the results shows the impact of the subsidy comparing just those who were measured to have “unmet need” at baseline in treatment versus control. Of these 4649 women (still a very large sample) the treatment women were only -.015 percent less likely to have a pregnancy, which is again practically very small and statistically not compellingly different from zero. The same is true for the women who at baseline reported not wanting another child over the next two years: impact of making contraception free does not reduce births.
These RCT results make perfect sense in the context of the Senderowicz and Maloney (2022) results that “unmet need” is not an expressed “need” or even a “demand” by women but a “need” inferred to/on women by demographers. The “demand side” reasons (women don’t want to use contraception for a variety of reasons having nothing to do with access or cost) are the dominant source of “unmet need.”
Which brings us to the question of whether the “unmet need” view really is the “most influential” or whether the authors were just setting up a straw man. My view is that the authors are sincere and correct, they are not setting up a straw man, the “unmet need” view is influential.
Which brings us to the interesting question: “Why is this view that fertility is independently causally driven to a large extent by “unmet need” due to lack of access, which is so easily refuted, nevertheless so influential?” I think two large parts of the answer are that: (a) demographically driven family planning advocates really do need it to be true and (b) Western donors love the narrative.
Those who thought that the “population bomb” was a terrible problem therefore wanted women, especially women in poor countries, to have fewer children to slow population growth. This easily led to coercive and near coercive actions to limit women’s fertility, which was a massive and damning moral failing of the movement (e.g. Matthew Connelly’s history Fatal Misconception). The way to reconcile the drive of demographers to limit women’s fertility with avoiding the charges of coercing women to do so is to claim that (i) women really wanted to reduce their fertility but (ii) their desire to limit fertility was inhibited by a lack of access to modern contraception. It is demographers (of a certain type) that have a need, and their need is to believe in “unmet need.” And as Upton Sinclair so succinctly puts it: “It is difficult to get a man to understand something, when his salary depends on his not understanding it.”
And people have salaries that depend on not understanding that “unmet need” is a bogus concept because donors love the narrative of “unmet need” because that means some relatively cheap thing is the key to great things (lowered fertility, better child health) and this means that modest amounts of funding to direct “interventions” can be believed to make a big difference, and this difference in good things for specific groups is directly attributable to the donor. What is not to love? So the family planning advocacy group Dupas et al (2025) mention in their AER article, FP2030 got a 1.4 billion, five year, commitment from the Bill and Melinda Gates foundation. That kind of money can keep a lot of people believing pretty much anything not matter what the data or even fancy RCTs say.